Indian Journal of Clinical Anatomy and Physiology
Indian Journal of Clinical Anatomy and Physiology (IJCAP) is an open access, peer-reviewed medical quarterly journal, published since 2014 under the auspices of the Innovative Education and Scientific Research Foundation (IESRF), which aims to uplift researchers, scholars, academicians, and professionals in all academic and scientific disciplines. we will be publishing articles ‘Ahead of Print’ immediately upon acceptance of manuscript. In addition, the journal allows free access (Open Access) to its contents, which is likely to attract more readers and citations to articles publishe...
The digital toll: Correlating nomophobia with perceived stress and sleep quality among first-year medical undergraduates
Abstract
Introduction: Nomophobia can be literally translated as ‘no-mobile-phone phobia’. It is the concern that people have when they cannot use their mobile phones or when they are separated from them. Nomophobic symptoms are especially prevalent among university students and significantly impact their quality of life, contribute to insomnia, affect academic performance, and increase symptoms of stress, anxiety and depression. So, to stress the need for intervention within the educational & clinical fields, we chose Nomophobia and its effect on sleep pattern and stress levels in medical students.
Materials and Methods: It is observational cross-sectional study in first year MBBS students. Respondents were selected on the basis of their willingness to participate in the study. Nomophobia questionnaire (NMP-Q), Perceived stress scale (PSS), The Pittsburgh Sleep Quality Index (PSQI) were used. The questionnaire was circulated in the form of google form. The students were informed that they’ll have to submit the mobile for 5-6 hours daily for 6 days. The data of NMP-Q, PSS & PSQI questionnaire were collected & analyzed.
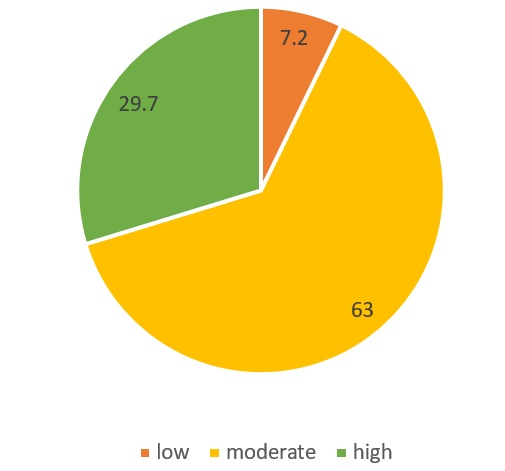
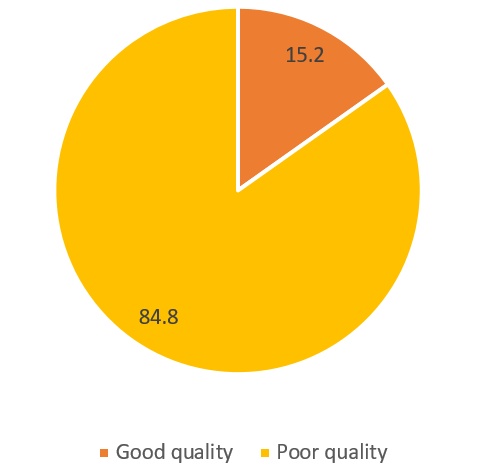
Result: The study highlights a high vulnerability among MBBS students to nomophobia (100% had nomophobia irrespective of the severity), which serves as a significant contributor to elevated stress levels (low-7.2%, moderate 63%& high 29.7%) and poor sleep hygiene. While perceived stress and nomophobia levels were comparable across groups, the retention of mobile devices was linked to significantly higher PSQI scores (13.66 vs 7.34), suggesting that nocturnal proximity to mobile devices is a primary driver of sleep disturbances in MBBS students, independent of their psychological stress levels.
Conclusion: The present study concluded that nomophobia is an emerging addiction. The overuse of the mobile can disturb the sleep pattern & increase the stress levels. Apart from other stressors, mobile phones have emerged as a significant additional stressor, which could be mitigated through more mindful usage of mobile phones.
1. Introduction
Mobile phones have become ubiquitous in modern society, with their use expanding far beyond basic communication. Initially designed to replace landline telephones and to facilitate communication on the move, mobile phones have now evolved into multifunctional devices that permeate nearly every aspect of daily life. Advances in digital technology, coupled with increased affordability, widespread availability, and reduced costs, have led to a dramatic rise in mobile phone dependency across populations worldwide, affecting individuals of all age groups and cultural backgrounds.[1]
Digital technologies have significantly transformed human lifestyles by enabling constant network access, rapid communication, collaboration, and online education. However, the escalating reliance on mobile devices has raised growing concerns, particularly regarding their excessive and maladaptive use.[2] In extreme cases, this dependence has progressed to behavioral addiction, giving rise to a condition known as nomophobia.[3] Nomophobia, literally meaning “no-mobile-phone phobia,” refers to the anxiety or distress experienced when individuals are unable to access or use their mobile phones or are separated from them.⁴,⁵ It has increasingly been described as an emerging psychiatric concern with potentially serious implications for social, mental, and physical health.[3][4]
Inappropriate and excessive mobile phone use has been shown to be particularly hazardous among school and college students. It has been associated with poor academic performance due to classroom distractions, decreased attention and concentration, impaired learning, and increased risk of accidents related to distracted driving.[1] Additionally, excessive mobile phone use may negatively impact interpersonal relationships by encouraging virtual interactions over face-to-face communication.[1] Nomophobia has been widely studied among university students across different countries and has been reported to adversely affect their overall quality of life.[6][7]
Recent empirical evidence indicates that nomophobia is associated with several adverse psychological outcomes, including increased levels of anxiety, stress, and depression, as well as insomnia and sleep disturbances.[8][9][10] Studies have also documented reduced attention span, impaired concentration, and diminished academic performance among individuals exhibiting high levels of mobile phone dependence.[11][12] These findings underscore the growing need to address nomophobia within both educational and clinical contexts.[13][14]
Previous research has identified various psychological and behavioral manifestations of nomophobia, such as frustration when unable to access a smartphone, a compulsive need to remain constantly connected, heightened stress during periods of separation from the device, and an uncontrollable urge to respond to calls or notifications—even during lectures or study hours.¹⁵ Such over-dependence on mobile phones has been shown to hinder concentration, learning efficiency, and productivity in academic environments.[16]
Sleep disruption is a particularly important consequence of excessive smartphone use. Studies have consistently shown that insufficient or poor-quality sleep adversely affects cognitive functioning, memory, emotional regulation, and overall academic performance. ¹⁷ Evidence suggests that nighttime smartphone use disrupts sleep patterns by altering circadian rhythms. Exposure to blue light emitted from mobile screens suppresses melatonin secretion, delays the biological clock, and ultimately reduces sleep duration and quality.[18][19]
Additionally, prolonged mobile phone use has been linked to various physical health complaints, including headaches, fatigue, stress, disturbed sleep, impaired memory (particularly short-term memory), reduced concentration, dizziness, sensations of heat around the ear, facial dermatitis, and emotional irritability.[1][20] In severe cases, excessive exposure has been associated with increased seizure frequency in children with epilepsy, hypertension, and potential long-term neurological risks.[1][20]
Understanding the prevalence of nomophobia and its association with factors such as sleep quality, perceived stress, depression, and academic performance is therefore crucial for educators, policymakers, and mental health professionals in order to develop effective preventive and intervention strategies.[16] Mobile phone dependence has been described as “possibly the biggest non-drug addiction of the 21st century,” highlighting the magnitude of this emerging public health concern.[21]
Although nomophobia and its associated outcomes have been increasingly studied, there remains a relative paucity of research specifically examining its relationship with perceived stress, particularly among medical students—a population known to experience high academic and psychological demands. Addressing this research gap may contribute valuable insights into the mental health implications of mobile phone dependence in this vulnerable group.
2. Aim
This study aimed to assess the level of nomophobia among MBBS students and to examine its association with sleep quality and perceived stress.
3. Objectives
3.1. Primary objectives
To determine the prevalence and severity of nomophobia among MBBS students. To assess sleep quality among medical students using a standardized instrument, the Pittsburgh Sleep Quality Index (PSQI). To measure perceived stress levels among medical students using a validated scale, the Perceived Stress Scale (PSS).
3.2. Secondary objectives
To examine the association between nomophobia and sleep quality, specifically whether higher levels of nomophobia are associated with poorer sleep quality. To evaluate the relationship between nomophobia and perceived stress, determining whether higher nomophobia scores correlate with increased perceived stress levels. To compare nomophobia scores across demographic variables, particularly gender. To identify potential predictors of high nomophobia among medical students, including duration of mobile phone use and ownership of mobile phones.
3.3. Study design and participants
This study employed an observational, cross-sectional design. Participants were recruited based on their willingness to participate in a study on nomophobia. All the 150 students were briefed on study objectives and procedure. Following this orientation, 138 students provided the consent and successfully completed the questionnaire.
Participants were informed that, as part of the study protocol, they would be required to submit their mobile phones to the department for 5–6 hours daily over a period of six consecutive days.
3.4. Inclusion criteria were
Ownership of a smartphone Willingness to participate and provide informed consent Willingness to submit mobile phones as per the study protocol
3.5. Exclusion criteria included
Presence of any diagnosed psychological or psychiatric disorder Current use of sleep-related medications.
Data collection was conducted after the completion of the second terminal examination, to minimize academic stress–related bias. Ethical clearance was taken from the institutional ethics committee.
3.6. Data collection tools
Data were collected using a structured questionnaire consisting of five sections:
Demographic details of the participants Mobile phone usage patterns Nomophobia assessment Perceived stress assessment Sleep quality assessment
The following standardized instruments were used:
3.6.1. Nomophobia questionnaire (NMP-Q)
Nomophobia was assessed using the Nomophobia Questionnaire (NMP-Q) developed and validated by Yildirim and Correia.[22] The NMP-Q consists of 20 items rated on a 7-point Likert scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Total scores range from 20 to 140 and are categorized as follows:
<20: No nomophobia 21–59: Mild nomophobia 60–99: Moderate nomophobia 100–140: Severe nomophobia
3.6.2. Perceived stress scale (PSS-10)
Perceived stress was measured using the Perceived Stress Scale (PSS-10) developed by Cohen et al. The scale consists of 10 items, with total scores ranging from 0 to 40, where higher scores indicate greater perceived stress. The PSS is a widely validated tool for assessing stress perception in various populations.
3.6.3. Pittsburgh sleep quality index (PSQI)
Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), a self-reported questionnaire that evaluates sleep quality over a one-month period. The PSQI comprises seven components, each scored from 0 to 3, yielding a global score ranging from 0 to 21. Higher scores reflect poorer sleep quality, and a global score >5 indicates poor sleep quality with high sensitivity and specificity.
3.7. Data collection procedure
The questionnaire was administered electronically using a Google Forms link, which was shared via the official departmental WhatsApp group. Participants completed the questionnaire on the last day of mobile phone submission. All responses were collected electronically and compiled for analysis.
3.8. Statistical analysis
Data were entered and analyzed using appropriate statistical software. Descriptive statistics were used to summarize participant characteristics, including frequencies, percentages, means, and standard deviations. Bivariate analysis was conducted using Pearson’s, chi-square test to examine associations between:
Nomophobia levels and sleep quality (PSQI) Nomophobia levels and perceived stress (PSS) Nomophobia scores and demographic variables such as gender and duration of smartphone use
A p-value of <0.05 was considered statistically significant.
4. Results
Result: Out of 138 students, 94 females and 44 males. The mean age of the participants was 19.4± 0.94 years. The study participants comprised of 31.9% males & 68.11% females.
Regarding smartphone ownership duration, 13.8% of the students had owned a smartphone for 10 years or more & 39.8% students possess their mobile for < 5years. Moreover, smartphone use of less than 2 hours per day was reported by 19.6% of students, while 21.7% reported usage of over 5 hours per day.
The above [Table 3] shows that nomophobia was significantly and positively correlated with perceived stress, indicating that higher levels of nomophobia are associated with increased stress. Furthermore, a significant positive correlation was observed between nomophobia and sleep quality scores, given that higher PSQI scores represent poorer sleep quality, this result suggests that increased nomophobia is associated with greater sleep disturbance.
Of the 138 students enrolled, 102 voluntarily submitted their mobile phones, while 38 did not (2 students joined the study later and did not wish to submit their mobile phones). Comparative analysis showed that nomophobia (NMP) scores were higher among participants than non-participants; however, the difference was not statistically significant. 53% of the study participants searched their mobile phones when it was submitted but the frequency reduced in 6 days to 81.4% participants later.
|
Female |
Male |
Total |
|
|---|---|---|---|
|
N |
94 |
44 |
138 |
|
∑X |
7613 |
3092 |
10705 |
|
Mean |
80.9894 |
70.2727 |
77.572 |
|
∑X2 |
664999 |
237970 |
902969 |
|
Std.Dev . |
22.8193 |
21.9337 |
23.0131 |
|
Duration of use |
Mild nomophobia |
Moderate Nomophobia |
Severe Nomophobia |
|---|---|---|---|
|
<2 hrs |
11 (6.26) [3.59] |
13 (16.24) [0.65] |
3 (4.50) [0.50] |
|
2-5 hrs |
18 (18.78) [0.03] |
52 (48.72) [0.22] |
11 (13.50) [0.46] |
|
>5 hrs |
3 (6.96) [2.25] |
18 (18.04) [0.00] |
9 (5.00) [3.20] |
|
Statistical Metric |
NMP-Q vs. PSS |
NMP-Q vs. PSQI |
|---|---|---|
|
Correlation Coefficient (r) |
0.3297 |
0.2624 |
|
95% Confidence Interval |
0.1721 to 0.4709 |
0.09963 to 0.4114 |
|
R squared (R 2 ) |
0.1087 |
0.06883 |
|
P-value |
< 0.0001 |
< 0.01 |
|
P-value Summary |
**** |
** |
An independent-samples t-test was conducted to determine if there were significant differences in sleep quality, nomophobia, and perceived stress between participants who submitted their mobile devices and those who did not.
There was a significant difference in sleep quality scores between the submission group and the non-submission group. These results suggest that participants who retained their devices experienced substantially higher levels of sleep disturbance. In contrast no significant difference was observed in nomophobia score.
|
NMP score (mean ±SD) |
PSS score (mean ±SD) |
Global PSQI score (mean ±SD) |
|
|---|---|---|---|
|
Participants who submitted their mobile |
76.5 ± 20.96189 |
21.03 ± 5.68465 |
7.34 ± 3.62471 |
|
Participants who did not submit their mobiles |
74.55 ± 26.54186. |
21.76 ± 6.82774 |
13.66 ± 6.13486 |
|
Low stress |
Moderate stress |
Severe stress |
Row Totals |
|
|---|---|---|---|---|
|
Male |
5 (2.87) [1.57] |
31 (29.46) [0.08] |
1 (4.67) [2.88] |
37 |
|
Female |
3 (5.13) [0.88] |
51 (52.54) [0.05] |
12 (8.33) [1.62] |
66 |
|
Outcome Variable |
r |
r2 |
p |
Significance |
|---|---|---|---|---|
|
Perceived Stress (PSS) |
.273 |
.074 |
.006 |
** |
|
Sleep Quality (PSQI) |
.275 |
.076 |
.005 |
** |
|
Outcome Variable |
r |
r2 |
p |
Covariance |
t-statistic |
|---|---|---|---|---|---|
|
Perceived Stress (PSS) |
.465 |
.216 |
.003 |
84.30 |
3.15 |
|
Sleep Quality (PSQI) |
.304 |
.093 |
.063 |
21.85 |
1.92 |
Pearson correlation coefficients indicated significant, weak-to-moderate positive relationships between nomophobia and both psychological metrics. NMP-Q scores were significantly correlated with perceived stress, p = .006, and sleep quality, p = .005. In this group, nomophobia accounted for approximately 7.4% and 7.6% of the variance in stress and sleep quality, respectively.
Association of Perceived stress & Sleep of the study participants
The f-ratio value is 420.94222. The p-value is < .00001. The result is significant at p < .05
Regarding the severity of nomophobia among non-participants, moderate levels were the most prevalent (52.6%), followed by mild (26.3%) and severe levels (18.4%). Minimal to no nomophobia was rare, accounting for only 2.6% of the group.
For the 38 individuals who did not submit their phones, there was a moderate, positive, and statistically significant correlation between nomophobia and stress (r = .465, p = .003). This suggests that within this specific group, as their nomophobia increases, their perceived stress rises sharply. Interestingly, while the correlation between nomophobia and sleep quality (r = .304) appears positive, it did not reach statistical significance.
5. Discussion
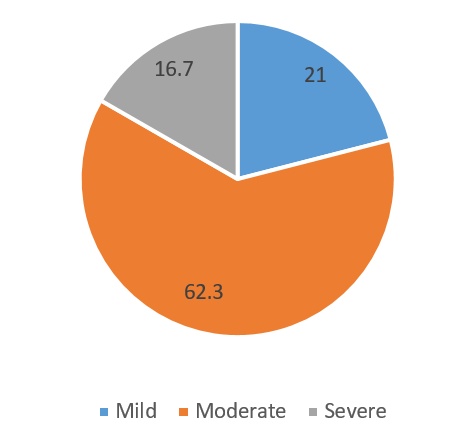
The present study analyzed nomophobia and its relation with perceived stress & sleep quality in 138 participants. It was demonstrated in our study that 100% of participants had fear of no mobile phone. The participants having moderate to severe nomophobia were more (76.8%), which corroborated with other studies also.[9][16][26]
5.1. Nomophobia and gender
The high prevalence rate of nomophobia among medical students is a problem that requires greater attention. Medical students, in particular, can be prone to nomophobia because they rely on their cell phones to meet the demands of academics and medical college.27 Nomophobia scores were higher among females than males; however, this difference was not statistically significant (as shown in table 1). Similar findings have been reported in other studies, where females consistently demonstrated higher nomophobia scores compared to male participants.[1][27]
One study found that females are more prone to anxiety related to smartphone use and disconnection, which can lead to higher levels of nomophobia. This may be attributed to social and emotional factors, as females tend to rely more heavily on smartphones for communication and social networking, heightening their fear of missing out (FOMO) and increasing their dependence on mobile devices. Similarly, other study reported that females are more vulnerable to nomophobia due to their higher emotional sensitivity to social disconnection.[28][29]
Conversely, several studies have indicated that nomophobia is equally prevalent across both genders.[25][30][31]
These findings indicate that gender-specific patterns of digital pathology are not monolithic. The prevalence of internalizing symptoms (e.g., anxiety) in females versus externalizing behaviors (e.g., excessive gaming) in males underscores a need for gender-sensitive diagnostic frameworks. Future longitudinal research is required to delineate how these disparate manifestations influence the long-term trajectory of technology-mediated dependencies.[32][33]
Evidence indicates that the gendered manifestation of nomophobia is contingent upon cultural and geographical landscapes. The heightened vulnerability observed in women within specific regions underscores the influence of environment on digital pathology. These findings necessitate a more nuanced, cross-cultural approach to understanding how gendered socializations influence the psychological stakes of connectivity.[34][35]
5.2. Nomophobia & duration of use
Statistical analysis (Table no-2) revealed that daily usage exceeding five hours serves as a critical threshold for increased nomophobia, whereas the total duration of device ownership remained non-significant. This distinction underscores that contemporary habits—rather than the length of time an individual has owned a mobile device—are the primary drivers of digital dependency and associated separation anxiety.[36][37]
5.3. Nomophobia & perceived stress
The significant association between perceived stress and nomophobia (p<0.0001) suggests that compulsive mobile phone proximity may exacerbate physiological and psychological stress responses. As R2 values reached as high as 0.4709, it is evident that nearly half of the variance in perceived stress can be linked to nomophobic behaviors in certain contexts. This relationship highlights the potential for digital dependency to diminish quality of life and serve as a catalyst for broader mental health challenges[9][26][32]
Many studies found that individuals with elevated levels of nomophobia were also associated with higher levels of stress.[37][38]
5.4. Nomophobia & sleep quality
The results of the current study reveal a significant correlation between nomophobia and poor sleep quality (R2=0.06883, p<0.0001), reinforcing a growing body of evidence that links digital dependency to sleep disturbances.[14][39][41]
While the statistical association is clear, the nature of this relationship appears to be more complex than a simple cause-and-effect model.
Our data is consistent with the findings which suggests the existence of a vicious cycle.[42]
The Catalyst: Excessive mobile phone use—driven by the anxiety of being disconnected—directly impairs sleep hygiene through blue light exposure and cognitive arousal.
The Feedback Loop: Conversely, the resulting sleep deprivation often leads to increased daytime phone reliance as a compensatory mechanism or a distraction from fatigue, which in turn further degrades sleep quality.[43]
This self-perpetuating loop underscores the necessity of a holistic intervention strategy. Rather than treating sleep issues or smartphone addiction in isolation, public health efforts for students must integrate sleep hygiene education with digital literacy and technological boundaries. Addressing one without the other likely leaves the underlying cycle intact.
5.5. Comparison between participants & Non- participants
Later on when the participants were required to submit their mobile phones, 38 students did not prefer to submit, probably indicating the fear of having no mobiles. The findings of the present study suggest that temporary restriction of mobile phone use did not result in a significant difference in nomophobia levels between participants and non-participants, although participants demonstrated slightly higher scores. Perceived stress levels were remarkably similar in both groups, indicating that stress may arise both from mobile phone deprivation and from continued mobile phone use. This convergence of stress scores suggests that mobile phones may act as both a stress-inducing and stress-alleviating factor, depending on context and individual reliance.
5.6. Stress correlation difference
Non-Participants (n=38): Had a much stronger correlation with stress (r = .465). This group's stress is intrinsically linked to their phone anxiety.
Participants (n=102): Had a weaker correlation (r = .273). Their stress may be influenced by a wider variety of life factors rather than just nomophobia.
In contrast, sleep quality differed significantly between the groups, with non-participants exhibiting higher PSQI scores, indicative of poorer sleep quality. This finding supports existing evidence that excessive or unrestricted mobile phone use, particularly during evening hours, may negatively impact sleep through mechanisms such as increased cognitive arousal, blue light exposure, and disrupted sleep routines. The improved sleep quality observed among participants may reflect the beneficial effects of reduced mobile phone exposure, even over a relatively short intervention period.
5.7. Sleep quality significance
Even though the r values are similar between groups (~.27 to .30), the relationship with sleep is statistically significant for the Participants but not significant for the non-participants
Why? The larger sample size (n=102) provides more statistical power to detect the relationship, whereas the non-submitters group (n=38) might require a much stronger effect to reach significance, or their sleep is so universally poor (M=13.66) that the NMP-Q score no longer predicts the variation well.
Overall, these results highlight the complex and dual role of mobile phone use in influencing stress and sleep outcomes. Exposure to blue light increases brain alertness and stimulates cognitive functions, resulting in poor sleep quality.[17][18][41] Another research with college students has suggested that the frequency of students to their mobile devices can be counterproductive because it has been found to cause cognitive overload thereby affecting the students’ ability to concentrate on their course work.[44]
6. Conclusion
This study compels that nomophobia is highly prevalent amongst all MBBS students with majority falling in moderate to severe category (76.8%). This underscores the risk of altering behavioral patterns within medical education.
PSQI scores when correlated with nomophobia proved that the students who temporarily surrendered their devices, reported significantly better sleep outcomes. This suggests that even a brief waiver period may confer remarkable sleep benefits.
A significantly linear correlation was observed between nomophobia and stress levels. Also, female medical students showed more vulnerability to mobile phone dependency linked to higher social networking as compared to their male counterparts.
The study highlights that it is the duration of usage rather than long term ownership of devices that drives its dependency.
So, to protect the mental and physical health of medical students, interventions must move beyond simple restrictions. Instead, a holistic approach is required—one that integrates digital literacy with sleep hygiene education to break the self-perpetuating loop of digital dependency.
7. Limitations
The present study has several limitations that should be considered when interpreting the findings. First, the relatively short duration of mobile phone restriction may not have been sufficient to produce measurable changes in nomophobia or perceived stress levels. Longer intervention periods may yield different outcomes. Second, the voluntary nature of participation introduces the possibility of self-selection bias, as individuals more motivated or confident in reducing mobile phone use may have opted to participate.
Additionally, reliance on self-reported measures may have introduced response bias, including social desirability and recall bias. Objective measures of mobile phone usage and sleep parameters, such as screen-time tracking applications or actigraphy, were not employed and could have strengthened the validity of the findings. The study also did not control for potential confounding factors such as caffeine intake, academic workload, or mental health status, all of which may influence stress and sleep quality.
Future directions interventional studies can be done aiming at sleep studies, measuring cortisol levels giving a better measurement of sleep and stress. Also measuring HRV could provide a better correlation between perceived stress and physical health of the MBBS students.
8. Acknowledgement
The authors would like to express sincere gratitude to the MBBS students who participated in the study. Their cooperation and willingness to submit their mobile phones for the study is highly appreciated and necessary for the completion of the study.
9. Conflict of Interest
None
10. Source of Funding
None.
References
- Mengi A, Singh A, Gupta V. An institution-based study to assess the prevalence of Nomophobia and its related impact among medical students in Southern Haryana, India. J Family Med Prim Care. 2020;9(5):2303-8. [Google Scholar] [Crossref]
- Luy-Montejo C, Medina Gamero AGLJ&TER. E. (2020). Nomofobia. Studium Veritatis. 2020. [Google Scholar] [Crossref]
- Rodríguez-García AM MALBJ. Nomophobia: An Individual’s Growing Fear of Being without a Smartphone-A Systematic Literature Review. Int J Environ Res Public Health. 2020;17(2). [Google Scholar] [Crossref]
- Bhattacharya S, Bashar M, Srivastava A, Singh A. NOMOPHOBIA: NO MObile Phone Phobia. J Fam Med Prim Care. 2019;8(4):1297-300. [Google Scholar] [Crossref]
- León-Mejía AC GMSIGJ. A systematic review on nomophobia prevalence: Surfacing results and standard guidelines for future research. PLoS One. 2021;16(5). [Google Scholar] [Crossref]
- Qutishat M, Rathinasamy Lazarus E, Razmy A, Packianathan S. University students’ nomophobia prevalence, sociodemographic factors and relationship with academic performance at a university in Oman. Int J Afr Nurs Sci. 2020;13. [Google Scholar] [Crossref]
- Kaur A, Ani A, Sharma A, Kumari V. Nomophobia and social interaction anxiety among university students. Int J Afr Nurs Sci. 2021;15. [Google Scholar] [Crossref]
- Sureka V, Abeetha S, Suma S, Subramanian S, Brinda S, Bhagyashree N. Prevalence of nomophobia and its association with stress, anxiety and depression among students. Biomedicine. 2020;40(4):522-5. [Google Scholar] [Crossref]
- Kubrusly M. Nomophobia among medical students and its association with depression, anxiety, stress and academic performance. Rev Bras Educ Med. 2021;45(3). [Google Scholar] [Crossref]
- Stanković M, Nesic M �S, Shi Z. Association of smartphone use with depression, anxiety, stress, sleep quality, and internet addiction: Empirical evidence from a smartphone application. Pers Individ Dif. 2021;168. [Google Scholar] [Crossref]
- Santhi V, Rajesh B. Impact of smartphone usage on the academic performance among medical students. J Evolution Med Dent Sci. 2020;9(02):105-10. [Google Scholar] [Crossref]
- Servidio R. Fear of missing out and self-esteem as mediators of the relationship between maximization and problematic smartphone use. Curr Psychol. 2021;40(1):1-11. [Google Scholar] [Crossref]
- Aldhahir A, Bintalib H, Alhotye M, Alqahtani J, Alqarni O, Alqarni A. Prevalence of nomophobia and its association with academic performance among physiotherapy students in Saudi Arabia: a cross-sectional survey. J Multidiscip Healthc. 2023;16:2091-2100. [Google Scholar] [Crossref]
- Guerra Ayala MJ AdlRO, Chambi Catacora M, Vargas Onofre E, Cari Checa E DFD. Nomophobia, phubbing, and deficient sleep patterns in college students. Front Educ. 2024. [Google Scholar] [Crossref]
- Mallya N SR, Mashal S. A study to evaluate the behavioral dimensions of “Nomophobia” and attitude toward smartphone usage among medical students in Bengaluru. Natl J Physiol Pharm Pharmacol. 2018;8(9):1553-7. [Google Scholar] [Crossref]
- Rehman W, Tehmina D, Noreen D, Almas S, Shamsi F, Abrar A. Nomophobia and Academic Performance: Exploring the Cognitive and Behavioral Impacts on University Students. Rev Res. 2024;9(2):149-61. [Google Scholar] [Crossref]
- Angelillo S, Sansone V, Paduano G, Lateano L, Di Giuseppe G, Nobile C. The quality of sleep: evaluation among university students. Front Public Health. 2023;11. [Google Scholar] [Crossref]
- Zhu W, Liu J, Lou H, Mu F, Li B. Influence of smartphone addiction on sleep quality of college students: the regulatory effect of physical exercise behavior. PLoS One. 2024;19(8). [Google Scholar] [Crossref]
- Copaja-Corzo C MBVDHMRMPE. Sleep disorders and their associated factors during the COVID-19 pandemic: data from Peruvian medical students. Medicina (Kaunas). 2022;58(10). [Google Scholar] [Crossref]
- Khan M. Adverse effects of excessive mobile phone use. Int J Occup Med Environ Health. 2008;21(4):289-93. [Google Scholar] [Crossref]
- Shambare R. Are mobile phones the 21st century addiction?. Afr J Bus Manage. 2012;6(2):573-7. [Google Scholar] [Crossref]
- Yildirim C. . Exploring the dimensions of nomophobia: Developing and validating a questionnaire using mixed methods research. 2014. [Google Scholar]
- Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385-96. [Google Scholar]
- Buysse D, Reynolds C, Monk T, Berman S, Kupfer D. The Pittsburgh Sleep Quality Index (PSQI): A new instrument for psychiatric research and practice. Psychiatry Res. 1989;28(2):193-213. [Google Scholar] [Crossref]
- Veerapu N, Philip R, Vasireddy H, Gurrala S, Kanna S. A study on nomophobia and its correlation with sleeping difficulty and anxiety among medical students in a medical college, Telangana. Int J Community Med Public Health. 2019;6(5):2074-9. [Google Scholar] [Crossref]
- Gupta D, Bhardwaj A, Prakash R, Jose N, Singh F. Nomophobia and its association with stress and coping styles among undergraduate students of a medical college in New Delhi: A brief analysis. Indian J Soc Psychiatry. 2024;40(3):267-74. [Google Scholar] [Crossref]
- Alkalash S, Aldawsari A, Alfahmi S. The Prevalence of Nomophobia and Its Impact on Academic Performance of Medical Undergraduates at the College of Medicine, Umm Al-Qura University, Makkah City, Saudi Arabia. Cureus. 2023;15(12). [Google Scholar] [Crossref]
- Yıldırım M ��. Fear of COVID-19 and smartphone addiction among Turkish adolescents: mitigating role of resilience. Fam J. 2022;30(4). [Google Scholar] [Crossref]
- Gezgin D, Hamutoglu N, Sezen-Gultekin G, Gemikonakli O. Relationship between Nomophobia and Fear of Missing out among Turkish University Students. Cypriot J Educ Sci. 2018;13(4):549-61. [Google Scholar] [Crossref]
- Basu S, Garg S, Singh M, Kohli C. Addiction-like behavior associated with mobile phone usage among medical students in Delhi. Indian J Psychol Med. 2018;40(5):446-51. [Google Scholar] [Crossref]
- Dixit S, Shukla H, Bhagwat A, Bindal A, Goyal A, Zaidi A. A study to evaluate mobile phone dependence among students of a medical college and associated hospital of central India. Indian J Community Med. 2010;35(2):339-41. [Google Scholar] [Crossref]
- Al Maghaireh D, Shawish N, Abu Kamel A, Kawafha M. Acute Nomophobia and Its Psychological Correlates in Adolescents: An Explanatory Sequential Mixed-Methods Approach. J Multidiscip Healthc. 2025;18:1445-60. [Google Scholar] [Crossref]
- Panova T, Etmova A, Berkovich A, Etmov A. How ICTs can influence psychological wellbeing: an analysis of uses and addiction potential. RSC Adv. 2020;10(40):24027-36. [Google Scholar]
- Al Ali N, Matarneh S. Exploring the role of smartphone use and demographic factors in predicting nomophobia among university students in Jordan. Int J Adolesc Youth. 2024;29(1). [Google Scholar] [Crossref]
- Ergin Z, Ozer A. Unravelling the Relation Between Fear of Missing Out, Time Spent on the Phone, Sex, Alienation, and Nomophobia. Psychol Rep. 2023;126(1):181-97. [Google Scholar] [Crossref]
- Anusuya G, Dinah H, Arumugam B, Karthik R, Annamalai R, Mani E. A Cross-sectional Study on Nomophobia among Undergraduate Medical Students in Chennai, India. J Clin Diagn Res. 2021. [Google Scholar] [Crossref]
- Göktaş A �A. The association between anxiety, activity performance and nomophobia in students. Sci Rep. 2025. [Google Scholar] [Crossref]
- Wolfers L, Festl R, Utz S. Do smartphones and social network sites become more important when experiencing stress? Results from longitudinal data. Comput Human Behav. 2020;109. [Google Scholar] [Crossref]
- Alzhrani A, Aboalshamat K, Badawoud A, Abdouh I, Badri H, Quronfulah B. The association between smartphone use and sleep quality, psychological distress, and loneliness among health care students and workers in Saudi Arabia. PLoS One. 2023;18(1). [Google Scholar] [Crossref]
- Guerra Ayala MJ AdlRO, Chambi Catacora M, Vargas Onofre E, Cari Checa E DFD. Nomophobia, phubbing, and deficient sleep patterns in college students. Front Educ. 2025. [Google Scholar] [Crossref]
- Rafique N, Al-Asoom L, Alsunni A, Saudagar F, Almulhim L, Alkaltham G. Effects of Mobile Use on Subjective Sleep Quality. Nat Sci Sleep. 2020;12:357-64. [Google Scholar] [Crossref]
- Mac Cárthaigh S, Griffin C, Perry J. The relationship between sleep and problematic smartphone use among adolescents: A systematic review. Dev Rev. 2020. [Google Scholar] [Crossref]
- Nguyen B, Nguyen N, Duong Le H, Nguyen L. Smartphone addiction and mental health problems among Vietnamese undergraduate students: the mediating role of sleep quality. Int J Ment Health. 2024;2024:1-23. [Google Scholar] [Crossref]
- Clayton R, Leshner G, Almond A. The extended iSelf: The impact of iPhone separation on cognition, emotion, and physiology. J Comput Mediat Commun. 2015;20(2):119-35. [Google Scholar] [Crossref]
- Abstract
- 1. Introduction
- 2. Aim
- 3. Objectives
- 3.1. Primary objectives
- 3.2. Secondary objectives
- 3.3. Study design and participants
- 3.4. Inclusion criteria were
- 3.5. Exclusion criteria included
- 3.6. Data collection tools
- 3.6.1. Nomophobia questionnaire (NMP-Q)
- 3.6.2. Perceived stress scale (PSS-10)
- 3.6.3. Pittsburgh sleep quality index (PSQI)
- 3.7. Data collection procedure
- 3.8. Statistical analysis
- 4. Results
- 5. Discussion
- 5.1. Nomophobia and gender
- 5.2. Nomophobia & duration of use
- 5.3. Nomophobia & perceived stress
- 5.4. Nomophobia & sleep quality
- 5.5. Comparison between participants & Non- participants
- 5.6. Stress correlation difference
- 5.7. Sleep quality significance
- 6. Conclusion
- 7. Limitations
- 8. Acknowledgement
- 9. Conflict of Interest
- 10. Source of Funding
- References
Article Metrics
- Visibility 253 Views
- Downloads 143 Views
- DOI 10.18231/j.ijcap.16518.1779963352
-
CrossMark

- Citation
- Received Date March 25, 2026
- Accepted Date May 28, 2026
- Publication Date June 30, 2026