Indian Journal of Clinical Anatomy and Physiology
Indian Journal of Clinical Anatomy and Physiology (IJCAP) is an open access, peer-reviewed medical quarterly journal, published since 2014 under the auspices of the Innovative Education and Scientific Research Foundation (IESRF), which aims to uplift researchers, scholars, academicians, and professionals in all academic and scientific disciplines. we will be publishing articles ‘Ahead of Print’ immediately upon acceptance of manuscript. In addition, the journal allows free access (Open Access) to its contents, which is likely to attract more readers and citations to articles publishe...
The anatomical variations of the calcaneal-talar facets in the Kongunadu population and their clinical implications
Abstract
Introduction: The calcaneus is the largest among the tarsal bones. It is stressed, particularly when walking and running in weight-bearing situations. The morphometric parameters of the calcaneum play a vital role during orthopedic procedures. The study's principal goals are to detect various talar facet configurations on the calcaneum's superior surface and to establish how talar facet configuration and calcaneal spur are related.
Materials and Methods: A cross-sectional, retrospective, observational study was done between August 2024 and December 2025 on 76 dry calcaneum bones obtained from the Department of Anatomy and Forensic Medicine.
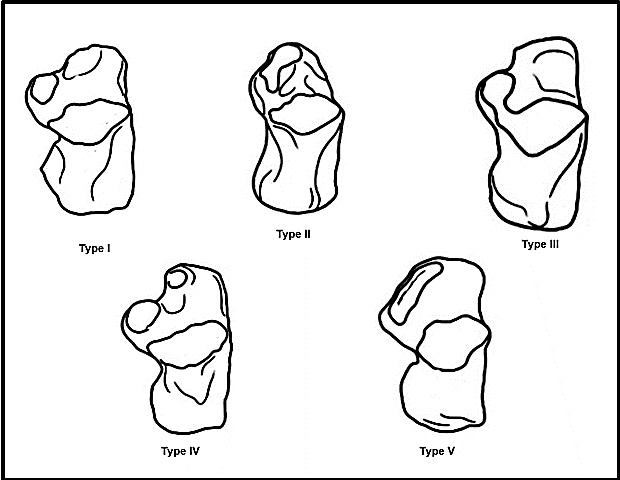
Results: We observed that out of 76 calcanei, 64.47% were of the Type I pattern with fused anterior and middle facets. 32.9% were of the Type II pattern with distinct anterior and middle facets. 2.6% of calcanei were of Type III, where there was an absence of anterior facets.
Conclusion: We observed that calcaneal spurs were related to the Type I pattern of facets in the highest frequency. Since calcaneal spurs are one of the most significant cofactors for heel pain, anatomical knowledge of the link between the calcaneal spurs and the pattern of calcaneal facets would be helpful in clinical treatment.
1. Introduction
The calcaneum, the biggest tarsal bone, serves as a brief lever for the calf muscles linked to its posterior aspect as it extends posteriorly to the tibia and fibula [1]. It has an upward slant and is oriented laterally and forward. It creates transverse tarsal joints and calcaneocuboid joints. The superior surface of the calcaneum has three facets where it articulates with the talus bone. They are facets that are anterior, middle, and posterior. The central facet is located on the sustentaculum tali, while the anterior and posterior facets are located on the body. There are significant differences in the quantity and configuration of these articular facets across different demographic groups.[2] The calcaneum's superior surface is separated into the following three regions. (a) The non-articular posterior third of the bone is rough and has a pad of fibrofatty tissue covering it that extends all the way to the tendocalcaneus. (b) A large oval facet—the posterior facet for the talus is seen in the middle third. (c) The middle and anterior facets for the talus are two articular facets that are present one-third more anteriorly.[3]
Researchers usually see changes in facet configuration as anatomical changes that have little functional impact. Bruckner (1987) asserts that subtalar joints produced by calcanei with pattern II facet configurations are less prone to arthritis and more stable.[4] There are two separate facets (anterior and middle) on the anterior third of the calcaneum, and the facets are configured using pattern II. Together with the posterior facet, the two facets form a "osseous tripod" that stabilizes the talus and limits the talar head's excessive mobility. By decreasing trauma and biomechanical stress on the subtalar joint, this tripod support lowers the risk of osteoarthritis, which is also less common in these situations. Because of their uneven weight distribution, unstable joints are more vulnerable to biomechanical stress, damage, and accidents.[5]. Since it is readily available and well-preserved, it is one of the bones utilized in forensic sciences.[6]
Solid, typically compact bones, the calcaneus and talus are commonly retrieved in circumstances where complete long bones may not be available.[7] The frequency of foot fractures is approximately two per 1,000 person-years for men and four per 1,000 person-years for women, making them the most common injury among people over 45.[8]
Calcaneal aspects might change as a result of heredity or postnatal variables, including gait and behaviors. The percentage distribution of the aspect’s pattern varies by sex and race, as was previously mentioned. Orthopaedic surgeons must comprehend the differences in calcaneal articular facets because they affect the stability of the subtalar joint while fixing foot deformities and placing screws for fracture fixation.
2. Materials and Methods
A cross-sectional retrospective observational study was done between August 2024 and December 2025 in which 76 calcanei were obtained from the Department of Anatomy and Forensic Medicine, Coimbatore, after obtaining ethical clearance from the institution.
2.1. Inclusion criteria
Undamaged and non-pathological calcaneum bones
2.2. Exclusion criteria
Damaged bones and structurally deformed bones.
Types of articular facets on the calcaneus were observed and classified by incidence of various patterns in percentages. The findings of the present study were compared with available literature.
3. Results
In the present study, 76 calcanei were studied based on gross features & classified into types and subtypes. Of the total 76 calcanei that were used for the study, 37 (48.68%) were right-sided and 39 (51.3%) were left-sided. Incidences of Types I, II, and III were shown in [Table 1] and 2. Type IV and V patterns were absent in the present study. Subtypes in Pattern I: Subtype A with fused middle and anterior facets are non-constricted (IA) in 25 bones and were found with a higher percentage (32.9%) compared to constricted (IB) in 24 bones (31.6%). The interfacet distance was measured using sliding calipers. The interesting finding of this study is the predominance of Type IA. In type II, subtype A with a narrow interfacet distance (< 2 mm) was found with 5.3%; subtype IIB (2-5 mm interfacet distance) was found with the highest (22.3%), and subtype IIC (> 5 mm interfacet distance) was found with the least percentage of about 7.9%.
|
Pattern |
Feature |
Right |
Left |
Percentage |
|---|---|---|---|---|
|
I |
Middle and anterior facets fused |
22 |
27 |
64. 47 % |
|
II |
Middle and anterior facets are separate. |
14 |
11 |
32.9 % |
|
III |
Anterior facet Absent |
1 |
1 |
2.6% |
|
IV |
Anterior, middle & posterior facets fused |
- |
- |
Nil |
|
V |
Middle & posterior facets fused |
- |
- |
|
Subtypes of calcaneum |
No. of bones |
Percentage |
|---|---|---|
|
Type IA |
25 |
32.9% |
|
Type IB |
24 |
31.6% |
|
Type II A |
4 |
5. 3 % |
|
Type II B |
17 |
2 2 .3% |
|
Type II C |
6 |
7.9% |
|
Study/ year |
Country/n=sample size |
Pattern I (%) |
Pattern II (%) |
Pattern III (%) |
Pattern IV (%) |
Pattern (V) |
|---|---|---|---|---|---|---|
|
Bunning and Barnett 1984 |
British /194 |
33% |
67% |
- |
- |
- |
|
Campos et al., 1989 [17] |
Spanish/176 |
53% |
46% |
- |
- |
- |
|
Verhagen 1993 [18] |
USA/ 191 |
54.45% |
26.7% |
18.85% |
- |
- |
|
G.S.Gindha et al., 2014 [14] |
North India /325 |
69.5% |
29.8% |
- |
0.6% |
- |
|
Dahkal Arun et al., 2018 [16] |
Nepal/142 |
56.34% |
42.25% |
- |
1.41% |
- |
|
Dang B et al., 2023 [13] |
North-west India/100 |
83% |
16% |
- |
1% |
- |
|
Jyotsna et al., 2022 [15] |
South india / 98 |
80.61% |
19% |
- |
- |
- |
|
Present study 2024 |
Kongu nadu population/76 |
64. 47 % |
32.9% |
2.6% |
- |
- |
|
Type of Calcanei |
No. of calcanei showing spurs |
Incidence of calcaneal spurs (%) |
||
|---|---|---|---|---|
|
plantar |
Dorsal |
Both |
||
|
Type I |
7 |
5 |
3 |
15 (19.7%) |
|
Type II |
1 |
0 |
1 |
2 (2.6%) |
|
Type III |
- |
- |
- |
- |
|
Type IV |
- |
- |
- |
- |
|
Type V |
- |
- |
- |
- |
|
Total no in (%) |
8 (10.5% |
5 (6.5%) |
4 (5.2%) |
17(22%) |
4. Discussion
Bunning & Barnett classified calcanei with 3 facets as type A, those with 2 facets as type B, and those with a single facet as type C. They noted that calcanei with 3 facets were predominant in European races, whereas Africans and Asians have calcanei with 2 facets. Racial differences and sexual dimorphism were identified in a fetal series, showing that they are most likely genetically determined. The same observations in the fetuses indicate genetic predisposition rather than the influence of walking patterns.[9] The observed ethnic differences may have a genetic or developmental basis because prenatal investigations have shown comparable talocalcaneal facet patterns. The biomechanical stressors and degenerative alterations observed in adults may also be influenced by functional factors including gait and weight-bearing patterns.[9] When comparing our findings with Bunning and Barnett, the present study observed 2 facets predominantly in type I A. The contrast may be because of racial differences. Gupta et al. classified the calcanei's facets into four classes. They discovered a prevalence of type I with nonconstricted facets (39%) in the Indian population.[10]
Sarvaiya et al. reported non-constricted facets due to the union of the anterior and middle facets to be observed in the majority (26% of calcanei) and the existence of a single joint facet to be the least (0.4%) [11]. Phunchago et al. investigated the articular facets on the calcanei in the Thai population and observed that the calcanei with a fusion of the anterior with the middle facet were present in the majority of continuous non-constricted facets in 35% and constricted facets in 33% of calcanei.[12] The current study's findings were similar to those of Gupta et al. and Sarvaiya et al., both of which studied the Asian population. However, Phunchago et al.'s findings are not identical to our study, which could be due to ethnic differences.
Based on the presence of talar facets on their superior surface, the calcanei have been divided into five categories. Numerous scholars have examined the prevalence of these categories in diverse populations. Of the 76 calcanei, we found that only 32.9% had a distinct anterior and middle facet and were of type II. Type I facets with merged anterior and middle facets were present in 64.47% of calcanei. Type III, or the lack of an anterior facet, is present in 2.6% of calcanei. According to Dang B et al. (2023), 16% of calcaneum out of 100 have a type II facet, whereas 83% have a type I facet, and 1% have a type III aspect.[13] The Type I facet outnumbered the Type II facet. Studies on the Indian race by G. S. Gindha et al. and Jyotsna et al.[14][15] and populations in Nepal, Spain, and the United States by Dhakal Arun et al., Campos F et al., and Verhagen FD are comparable.[16][17][18] Compared to Type I, which had a population of 37% and 25%, Type II had a higher population of Americans and Belgians (46% and 64%, respectively). Our study's findings are comparable to those of Dang B et al.'s study on the Indian population, which found 1% type III calcaneum.[13]
A number of authors study the calcanei in order to see the articular facet pattern. The talus's articular facets were divided into four groups by Bruckner: A (three facets), B (transitional two facets), C (simple two facets), and D (special two facets). The talus and calcaneus move more easily and in unison when there are two facets instead of three. The stiff foot that results from the three-facet shape is more prone to subtalar joint disorders. Those with two facets benefit more from physiotherapy than those with three.[4] This study shows that the number of subtalar joint facets affects foot mobility to the extent that osseous factors indicate joint range of motion. A continuous or single medial facet raises the risk of developing subtalar arthritis, according to Drayer-Verhagen.[18] These characteristics cause ligaments to become loose and joints to become unstable.
Four classes of articular facets are included in the Type A categorization. A1: Less than 2 mm separates the anterior and middle articular facets. A2: There is a 2–5 mm gap between the anterior and middle articular surfaces. The distance between the anterior and middle articular facets in A3 is greater than 5mm.
One joint facet is referred to as the anterior talar facet (A4). Type B combines the anterior and middle characteristics of two types (B1 and B2. The anterior and center sides of B1 were found to be constricted. B2: The middle and anterior aspects are not constricted.
C:When all three facets are combined, a single aspect is produced.Combining the anterior, middle, and posterior facets.Type A is related to type II, type C to type IV, and type B to type I.[9][19]
In the present, we observed that among type I articular facets, subtype IIB was the most prevalent, with an interfacet distance of 25 mm. These results align with those of Kullar et al. and Muthukumaravel et al. in the Indian population [20][21]. Type I individuals with fused anterior and middle facets may have a higher risk of developing subtalar arthritis.[22]
Dogan anatomic reduction, soft tissue relaxation, and osteotomy are the most successful for complicated foot abnormalities. Restoring a normal-sized, pain-free, and functional foot is the main aim. A sound treatment strategy can be developed with an understanding of the anatomy of the foot. The triple arthrodesis method requires meticulous examination of the calcaneum’s articular configuration in order to restore the flat foot. This guarantees the complete removal of cartilage from the subtalar joint surfaces.[23] Advancements in subtalar implants, flaps, and foot prostheses have been made possible by technology. The treatment procedures will be built upon comprehensive anatomical data.[24] The facet surfaces of the talus and calcaneus can be seen using 3D digital imaging. The diagnosis and treatment of coalition, talocalcaneal subluxation,and other dysmorphologies would be more successful as a result. Furthermore, joint implants and prosthetics may be created.
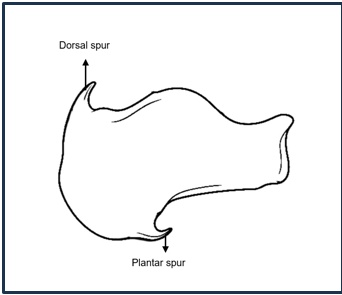
The incidence of calcaneal spurs was 22% in the present study, which is greater than Kori et al.[25] in Uttar Pradesh but comparable to Biswal R. et al.[26] Because the fused surface modifies normal subtalar joint mechanics, the type I calcaneal facet pattern, in which the anterior and middle facets are fused, may enhance the production of calcaneal spurs. During walking and standing, this fusion concentrates compressive stresses on the calcaneus and lessens independent movement across aspects. Calcaneal spurs are more common as a result of reactive bone growth at the calcaneal attachment sites brought on by increased stress and plantar fascial tension.[27] Last but not least, plantar spurs were more common in Type I calcanei (4%) and Type II calcanei (2.5%), with a total incidence of 6.5%,according to Kullar et al.[20]. Type III and IV calcanei showed no signs of plantar spurs (Tables 4, 5, Figure. 1).
|
Study / year |
No. of calcanei studied |
Plantar spurs (%) |
Dorsal spurs (%) |
Both spurs (%) |
Total spurs (%) |
|---|---|---|---|---|---|
|
Kull a r et al. (2013) [20] |
200 |
6.5 % |
15.5 % |
4.5 % |
26.5 % |
|
Kori et al. (2016) [25] |
600 |
60.4% |
35 % |
4.7 % |
17.7 % |
|
Biswal R et al., (2017) [26] |
107 |
18.7 % |
10.28 % |
4.7 % |
33.68% |
|
Present study (2024) |
76 |
10.5 % |
6.5 % |
5.2 % |
22 % |
5. Conclusion
Fused talar facets may change subtalar biomechanics and increase vertical compressive stress on the heel, as indicated by the greater frequency of plantar calcaneal spurs in Type I calcanei. Therefore, rather than being exclusively a result of plantar fascial tension, calcaneal spurs may be an adaptive reaction to persistent mechanical pressure. The clinical assessment and treatment of heel pain may benefit from an understanding of the connection between calcaneal facet morphology and spur development.
6. Limitations
Compared to bigger Indian investigations, the study was constrained by a rather small sample size (n=76). Evaluation of sexual dimorphism and age-related changes was also hindered by the dried calcanei's lack of age and sex information.
7. Acknowledgement
We sincerely acknowledge the contribution of Kirthi Sankar M., a Phase III, Part 1 student, who assisted in preparing the anatomical illustrations and diagrams used in this paper. Her effort and support greatly enhanced the visual presentation of the study.
8. Source of Funding
None.
9. Conflict of Interest
None.
References
- Standring S, Ellis H, Healy J, Johnson D, Williams A, Collins P, et al. Gray’s anatomy: the anatomical basis of clinical practice. 39th ed. 2005;26(10):2703-4. [Google Scholar]
- Datta A. Essentials of human anatomy. Current Books International. 2017. [Google Scholar]
- Singh V. Textbook of Anatomy: Abdomen and Lower Limb; Volume II. Elsevier Health Sciences. 2018. [Google Scholar]
- Bruckner J. Variations in the human subtalar joint. J Orthop Sports Phys Ther. 1987;8:489-94. [Google Scholar] [Crossref]
- Lawrence B, Buckner G, Mirka G. An adaptive system identification model of the biomechanical response of the human trunk during sudden loading. J Biomechanical Eng. 2006;128(2):235-41. [Google Scholar] [Crossref]
- Kidd R, Oxnard C. Patterns of morphological discrimination in selected human tarsal elements. American Journal of Physical Anthropology: The Official Publication of the. Am Assoc Physical Anthropol. 2002;117(2):169-81. [Google Scholar] [Crossref]
- Holland T. Estimation of adult stature from the calcaneus and talus. Am J Physical Anthropol. 1995;96(3):315-20. [Google Scholar] [Crossref]
- Melton III L. . In Osteoporosis in Men. 1999. [Google Scholar]
- Bunning P, Barnett C. A comparison of adult and fetal talocalcaneal articulations. J Anat. 1965. [Google Scholar]
- Gupta S, Gupta C, Arora A. Pattern of talar articular facets in Indian calcanei. J Anat. 1977;124:651-5. [Google Scholar]
- Sarvaiya B, Patel S, Single G, Master D. Morphometric measurements of the human calcaneum bone, the types of talar articular facets, and morphometric measurements of the human calcaneum bone of the Gujarat region. NJIRM. 2012;3:975-9840. [Google Scholar]
- Phunchago N, Uabundit N, Chaisiwamongkol K, Chaichun A, Iamsaard S. Types and morphometric study of calcaneal articular facets on human talus of Thai population. Int J Morphol. 2018;36:975-8. [Google Scholar]
- Dang B, Rathee S, Gupta S, Vashist Y. Morphometric Analysis of Variations in Pattern of Talar Articular Facets on Calcaneum in North-West India. J Indian Acad Forensic Med. 2023;45(2):112-5. [Google Scholar] [Crossref]
- Gindha G, Kaur H, Kaushal S, Singh M. Variations in the articular facets on superior surface of calcaneus in North Indian population: A Dry Bone Study. Hum Bio Rev. 2015;4(1):27-37. [Google Scholar]
- Jyotsna G, Mamidi A. The morphometric analysis of the calcaneus and its articular facets. Indian J Clin Anat Physiol. 2022;9(1):22-4. [Google Scholar] [Crossref]
- Dhakal A, Adhikari P, Khan A, Gautam A. Patterns of superior articular facet and morphometric study of Nepalese dry calcanei. Sanamed. 2018;13(1):17-22. [Google Scholar] [Crossref]
- Campos F, Pellico G. Talar articular facets (facies articulares talares) in human calcanei. Cells, Tissues, and Organs. 1989;134(2):124-7. [Google Scholar] [Crossref]
- Drayer-Verhagen F. Arthritis of the subtalar joint associated with sustentaculum tali facet configuration. J Anat. 1993. [Google Scholar]
- Boyan N OEKE, Soames R, Oguz O. Morphometric Measurement and Types of Articular Facets on the Talus and Calcaneus in an Anatolian Population. Int J Morphol. 2016;34(4):1378-85. [Google Scholar] [Crossref]
- Kullar J. Morphology of talar articular facets of calcaneus and its clinical implications. Kashmir J Med Sci. 2015;15(1):10-4. [Google Scholar]
- Muthukumaravel N, Ravichandran D, Melani Rajendran S. Human calcaneal facets for the talus: Patterns and clinical implications. J Clin Diagn Res. 2011;5(4):791-4. [Google Scholar]
- Greer Richardson E e. . 9th ed. 1998. [Google Scholar]
- Dogan A, Albayrak M, Akman Y, Zorer G. The results of calcaneal lengthening osteotomy for the treatment of flexible pes planovalgus and evaluation of alignment of the foot. Acta Orthop Traumatol Turc. 2006;40:356-66. [Google Scholar]
- Garg R, Dagal N, Kumar S, Shekhawat S. Original article Study of patterns of talar articular facets of human calcanei and their clinical implications in population of Rajasthan. Ind J of Basic App Med Res. 2013;7:643-50. [Google Scholar]
- Deepshikha K, Ganpat P, Archana R, Rakesh KD, Ritu S, Pooja S. Study of Variations In Talar Articular Facets Of Human Calcanei And Their Association With Calcaneal Spurs In North Indian Population. Int J Anat Res. 2016;4(3):2710-6. [Google Scholar]
- Biswal R, Mishra D. N, Mohapatra C. Study Of Calcaneal spurs On the Basis of Talar Articular Facets In the population of Odisha. Int J Anat Res. 2018. [Google Scholar]
- Ananthakrisnan R, Chitra R, Kumaravel S, Thenmozhi M. Subtalar joint instability and calcaneal spurs associated with the configuration of the articular facets of adult human calcaneum in Indian population. J Clin Diagn Res. 2016. [Google Scholar] [Crossref]
Article Metrics
- Visibility 216 Views
- Downloads 151 Views
- DOI 10.18231/j.ijcap.16880.1779963712
-
CrossMark

- Citation
- Received Date April 15, 2026
- Accepted Date May 27, 2026
- Publication Date June 30, 2026