Panacea Journal of Medical Sciences
Panacea Journal of Medical Sciences (PJMS) open access, peer-reviewed triannually journal publishing since 2011 and is published under auspices of the “NKP Salve Institute of Medical Sciences and Research Centre”. With the aim of faster and better dissemination of knowledge, we will be publishing the article ‘Ahead of Print’ immediately on acceptance. In addition, the journal would allow free access (Open Access) to its contents, which is likely to attract more readers and citations to articles published in PJMS.Manuscripts must be prepared in accordance with “Uniform requiremen...

Study on the seroprevalance rate of leptospirosis in tertiary care hospital, Kolkata
Abstract
Background: Leptospirosis is a worldwide prevalent septicemic zoonotic disease caused by spirochaetes Leptospira having wide spectrum of illness. Animals particularly rats are the main reservoir of disease and is mainly transmitted with contaminated rain water infected with rat urine. The organisms enter our body through cuts & abrasions. The disease presents with diverse clinical presentations making confusion with other febrile illnesses.
Aims & Objectives: The present study was undertaken to determine sero-prevalence & seasonal trends of Leptospirosis in surrounding locality of our hospital.
Materials and Methods: This is a prospective cross-sectional study conducted at the Department of Microbiology for 1 year from January to December 2023. The inclusion criteria is patients with febrile illness more than 5 days. A total of 571 blood samples were received for Leptospira serology. Centrifuged serum sample were tested by Pan bio-ELISA KIT for qualitative detection of IgM antibody to Leptospira.
Results: Amongst 571 received sample, 75 samples (13.13%) were serologically reactive by ELISA. Most of the positive cases clinically presented with fever and headache and were admitted in medicine ward. Highest seroprevalence was found more in male patients (53.3%) and in 21 to 40 years of age groups (29.3%). Period from July to September month noted to have highest prevalence.
Conclusions: This study gives an idea of seropositivity rate about Leptospira in the surrounding locality of our hospital in Central Kolkata. Improvement of hygiene and sanitation can prevent transmission. Increased awareness and early diagnosis and treatment can reduce the treatment cost, morbidity and mortality.
Introduction
Leptospirosis, a septicemic zoonotic disease which has worldwide distribution with a much greater incidence in tropical countries, is caused by the pathogenic spirochete Leptospira interrogans. The spectrum of illness is extremely wide, ranging from undifferentiated febrile illness to severe multisystem complications like renal failure and jaundice. Onset is usually sudden, with symptoms including headache, fever, muscle pains, conjunctival suffusion, meningitis and abdominal pain. The disease is caused mainly by carrier animals with chronic renal infection such as rodents, cattle, sheep, goat, etc., who excrete the organisms in their urine, contaminating the environment.[1] Man is an accidental host in leptospirosis infected through direct or indirect contact of cuts or abrasions in skin and mucosa with infected urine or tissues of carrier animals or, more commonly by indirect exposure to the organisms in damp soil or water.[2] In the city of Kolkata, in West Bengal, there is a high average rainfall with water holding capacity of soil. Here uncontrolled increase in rodent and stray dog population are main factors to increase the reservoir of the disease, poor sanitary conditions of roadside slaughtering stations having equal contribution for spread of this disease. The natural water reservoirs in and around the city are frequently used for bathing, swimming and watering of both man and animals. All these factors predispose this area for the persistence of leptospira outside and inside the host, and thus, humans are being affected every year producing a serious health hazard. [3] During the recent times the prevalence of the disease have been reported from various parts of the country,[4], [5] but the true incidence of cases in West Bengal is not known because of the lack of awareness, or the lack of diagnostic techniques.[3], [6] Moreover, people of this part of the globe suffering from infectious jaundice are sometimes mistreated as a case of viral hepatitis. Therefore, the present study had been undertaken at our tertiary care hospital to determine the prevalence and seasonal trends of Leptospirosis in this part of Kolkata so that we can awaken awareness among clinicians for proper diagnosis and early treatment to prevent complications and mortality from the disease.
Aims
To determine the seroprevalence of Leptospirosis amongst febrile patients who attended OPD and IPD of medicine department at CNMCH and to evaluate the seasonal trends of Leptospirosis.
Materials and Methods
Study design
The present study is prospective cross-sectional study.
Data collection
After approval by the ethical committee data has been collected for 1 year.
Place of study
Department of Microbiology, Calcutta National Medical College & Hospital Period of study: One year from January to December 2023.
Study population
Blood sample from suspected leptospirosis patients were sent to the microbiology laboratory irrespective of all ages and sexes from OPD and IPD of fever clinic and medicine wards. Relevant history was collected from the patients and their relatives.
Informed consent was also taken from each patient or his/her near relative while collecting blood for the study purpose.
Sample
In present study 570 samples has been taken for 1 year.
Inclusion criteria
All the blood samples with acute febrile illness with less than 5 days duration.
Study procedure
The received serum samples were tested for the specific anti-Leptospira antibodies using IgM ELISA KIT. Serum was separated and stored at -20 C until tested. It has been centrifuged at 3000 rpm for 5 minutes. Then centrifuged serum samples were tested for specific anti Leptospira IgM antibodies against Leptospira genus specific antigen by MAC ELISA by using Pan-bio-IgM ELISA kit. The uses of icteric sera or sera exhibiting haemolysis, lipemia or microbial growths were rejected. Required number of microwells had been taken, and then 10µl of patient serum added with 990 µl of sample diluent in a vial. Then 100 micro litre of diluted patient serum, positive & negative control and calibrators had been taken into their respective microwells.
After 30 min incubation it was washed six times with diluent buffer. Then 100 µl HRP conjugated Anti human IgM added into each well followed by 100 µl of each of TMB substrate and stop solution.
Presence of significantly raised level of IgM is a considered as presumptive evidence of active Leptospira infection.
Calculation
Calculation has ben done by following steps:
The average absorbance of the calibrator in triplicate was calculated and multiplied by calibrator factor provided with the kit, to determine the cut off value.
Index value was calculated by dividing the sample absorbance by cut off value.
Pan-bio unit was calculated by multiplying the index value by 10.
The test results were interpreted as Pan Bio units according to the manufacturer’s protocol.
Values less than 9 Pan bio units were considered as negative, 9-11 equivocal, and greater than 11 as positive. Equivocal samples had been retested after 10 days. Sensitivity of Pan-bio-ELISA Kit is 88-99% and specificity is 95-99% as mentioned in the kit literature.
Statistical analysis plan
Data has been presented by appropriate tables, graphs and charts.
Results
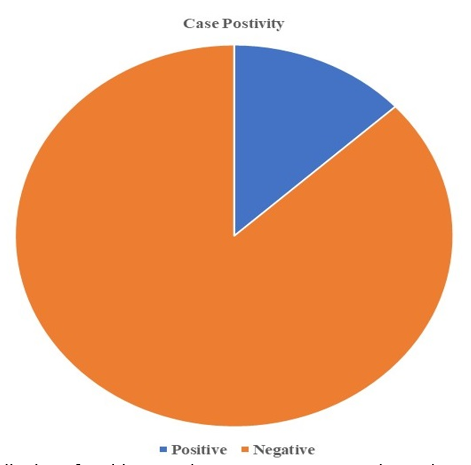
Amongst total 571 received samples from patients 75 samples (13.13%) were serologically reactive by ELISA ([Figure 1]).
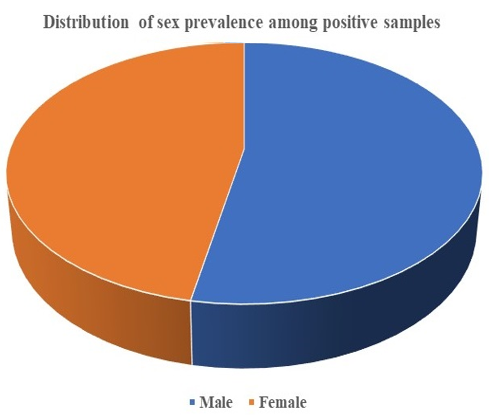
Amongst the positive cases, 40 (53.3%) were male and 35 (46.7%) were female ([Figure 2]).
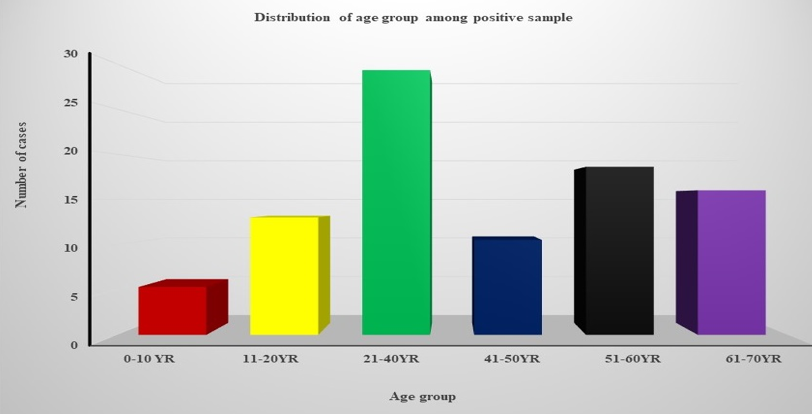
Highest prevalence of seropositivity (29.3%) was found in 21 to 40 years of age group and (18.6%) samples belonged to 51-60 years of age group. The remaining cases were distributed in the following age groups like - (16%) in 61-70 years age groups, (13%) in 11-20 years age group, (10.5%) samples belonged to 41-50 yrs. age group and (5.3%) in less than10yrs age group. ([Figure 3]).
Most of the positive cases 37% (n=28) presented with fever along with headache followed by fever with myalgia in 31.3 % (n=25), 13% (n=10) cases presented with jaundice, 2.6% (n=2) cases admitted in Intensive care unit for Hepatic Renal complications and 4% (n=3) cases out of 75 presented with convulsions ([Table 1]).
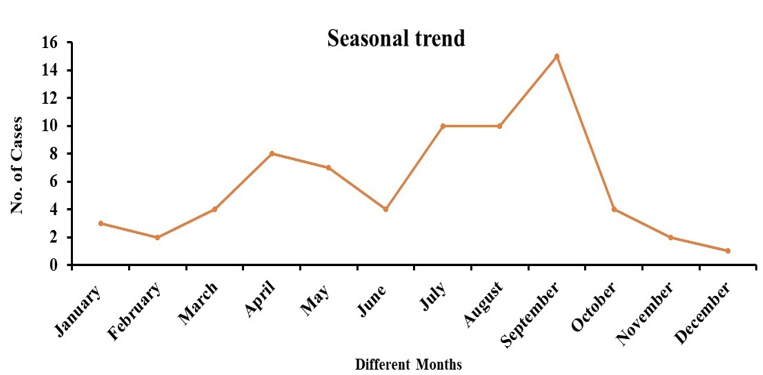
The period from July 2023 to September 2023 was noted to have the highest prevalence. (46.5%) samples were positive in this period ([Figure 4]).
|
Fever with headache |
28 (37%) |
|
Fever with myalgia |
25 (31.3%) |
|
Convulsion |
3 (4%) |
|
Jaundice |
10 (13%) |
|
Hepatomegaly |
1 (2%) |
|
Renal failure |
1 (2%) |
Discussion
The present study had undertaken to determine the seroprevalence of leptospira in and around our hospital locality (Park Circus) area by using Pan-bio-ELISA Kit. This kit has Leptospira biflexa Pantoc I strain as a standard. Sensitivity of Pan bio-IgM ELISA kit has been reported to be 76-90%. [6] IgM antibody appears as early as 1 week of illness reaches peak within 3rd to 4th weak & becomes undetectable after 6 months.[6] Therefore, we selected the patient who had history of fever more than 7 days. Out of total 571 samples 75 samples were seropositive (13.13%). None of the sample shows cross reactive antibodies after recall the patient during convalescent stage within 2 weeks. Similar other studies like De et al, 2002,[7] following post flood outbreak at Mumbai in 2002 showed positivity rate 36% In other Indian study Chandra Sekhar et al,1995 & Babu et al, 2001[8], [9] IgM ELISA positivity was 41.77% and 88.9% respectively. In other local studies from Kolkata Mandal et al reported 52.97% in post monsoon periods (2011) & Majumdar et al., 2013, 36% respectively. Sethi et al. reported in a retrospective study (2004-2008) in North India an increased incidence of Leptospirosis from 11.7% in 2004 to 20.5% in 2008.[4] A study from South India (Coimbatore) during 2007-2009 reported a total of 215 cases.[10] Between the year 2001 and 2009, 70-80% cases of Leptospira infections were reported in Gujrat. Andaman & Nicobar Island one of the most endemic areas in the world has documented incidence rate of 50/one lakh population.[11] This disease also reported worldwide like West pacific areas, Sri Lanka, Thailand, Indonesia, New Zealand etc.[9] Our prevalence is slightly less compared to other studies may be due to less rainfall in that particular season.
Apart from IgM ELISA, dark ground microscopy is a simple economical method of early diagnosis of Leptospirosis. Sensitivity of this test varies from 27% to 40%. MAT (Microscopic agglutination test) is also a reference test for Leptospirosis but it has limitation like it is inadequate for rapid case detection as it required paired sera for testing as well as it can be performed in few referral laboratories. Moreover prevalent serovars in a particular geographical area must be known to perform that test hence it is cumbersome to test 200 serovar of L. interogens. Several rapid tests like dipstick had come for screening for actually ill patient.[12] According to these study leptospira occurred mostly in active working population of age group 20 to 40 years. Also, occupational exposure, mostly were outdoor workers like sewage worker, butcher, farmer rather than student and house wife. Male predominance was more (53.3%) then female (46.7%) can be attributed for frequent outdoor activity. These all facts had corroborated in other study like Majumdar et al. 2013, Mondal et al., 2011 & Vimala et al., 2014.[6], [12], [13] According to NICD report, highest prevalence rate of leptospirosis was noticed in several states and union territories including West Bengal. [14] Particularly it was recorded from Kolkata, in 2007 on post monsoon period (September-October); the children (age group 5-10 years) were mostly (27.57%) affected with higher number of males. In Orissa, the incidence was higher (5.95%) among males in the age group of 6-15 years.[15] In Northern India, the mean age of patients was 32.6 years, and males predominance (57%) was higher than females (43%) with a peak during the rainy season.[4] All those findings are corroborative with our study.
The commonest clinical presentation of our study was fever with headache (37%), fever with myalgia (31.3%),and jaundice (13%) similar prevalent sign and symptoms were observed in study by Prabhu et al., 2010[16] were fever with headache (100%), arthralgia (56%) and jaundice (35%) were notice,
Most of the cases clustered around Beniapukur area, favours that urban slum with inadequate sanitation facilities also contribute to spread of disease. As antibody titre start rising after 1 week, so empirical treatment with doxycycline, ceftriaxone should be started once clinical suspicion set in, otherwise there may be chance of organ failure in further course of disease. [17] Documenting high level of seroprevalences amongst rodents, it is also important to aware the general public the need for rodent control and use of protective barrier for farmers as important method to control Leptospirosis.
Conclusion
In this study we used ELISA to study seroprevalence of leptospirosis. This study gives an idea of seropositivity rate about Leptospirosis. Highest seropositivity was found during rainy season. So, improvement of hygiene and sanitization has led to the decrease in seroprevalence rates of leptospirosis. This neglected disease must be dealt with high index of suspicion both in diagnosis and treatment as it may give rise to life threatening complications.
Source of Funding
None.
Conflict of Interest
None.
References
- Dutta T, Christopher M. Leptospirosis-an overview. J Assoc Physicians India. 2005;53:545-51. [Google Scholar]
- Unnikrishnan D, Pisharody R, Vijayalakshmy N. Prognostic Factors in Leptospirosis A Study From Kerala, India. Infect Dis Clin Pract. 2005;13(3):104-7. [Google Scholar]
- Debnath C, Pal N, Pramanik A, Biswas M. A serological study of leptospirosis among hospitalized jaundice patients in and around Kolkata. Indian J Med Microbiol. 2005;23(1):69-9. [Google Scholar]
- Sethi S, Sharma N, Kakkar N, Taneja J, Chatterjee S, Banga S. Increasing trends of leptospirosis in northern India: a clinico-epidemiological study. PLoS Negl Trop Dis. 2010;4(1). [Google Scholar] [Crossref]
- Basu D, Sarkar P, Chakraborty N, Chanda P, Biswas S, Bera B. Leptospirosis and Weil's disease in eastern India. J Indian Med Assoc. 2003;101(9):532-6. [Google Scholar]
- Majumdar M, Bhaduri A, Mandal M, KHaldar. A study on serological correlation of clinically suspected leptospirosis cases in West Bengal, India. Ann Trop Med Public Health. 2013;6(1). [Google Scholar] [Crossref]
- De A, Varaiya A, Pujari A, Mathur M, Bhat M, Karande S. An outbreak of leptospirosis in Mumbai. Indian J Med Microbiol. 2002;20(3):153-5. [Google Scholar]
- Chandrasekaran S, Mallika M, Pankajalakshmi V. Studies on the incidence of leptospirosis and possible transmission of Leptospira during leptospiraemia. Indian J Pathol Microbiol. 1995;38(2):133-7. [Google Scholar]
- Babu S, Pisharody R. Leptospirosis-experience in an epidemic. . 2001. [Google Scholar]
- Prabhu N, Innocent D, Chinnaswamy P. Thrombocytopenia in leptospirosis and role of oral amoxicillin and doxycycline for patient management. Int J Pharm Sci Bio. 2010;1:25-9. [Google Scholar]
- Pappas G, Papadimitriou P, Siozopoulou V, Christou L, Akritidis N. The globalization of leptospirosis: worldwide incidence trends. Int J Infect Dis. 2008;12(4):351-7. [Google Scholar]
- Debmandal M, Mandal S, Pal N. Serologic evidence of human leptospirosis in and around Kolkata, India: a clinico-epidemiological study. Asian Pac J Trop Med. 2011;4(12):1001-6. [Google Scholar]
- Vimala G, Rani A, Gopal V. Leptospirosis in vellore: a clinical and serological study. Int J Microbiol. 2014. [Google Scholar] [Crossref]
- Joseph A, George D. Epidemiology of leptospirosis-Kerala Scenario. Eur J Epidemiol. 2010;3(4):119-21. [Google Scholar]
- Pappas G, Papadimitriou P, Siozopoulou V, Christou L, Akritidis N. The globalization of leptospirosis: worldwide incidence trends. Int J Infect Dis. 2008;12(4):351-7. [Google Scholar]
- Prabhu N, Joseph P, Chinnaswamy P. Seroepidemiological trends of human leptospirosis in Coimbatore, India between 2007 and 2009 . Adv Appl Sc Res. 2007;1(1):113-9. [Google Scholar]
- Levett P, Haake D. Leptospira species (leptospirosis). Principles and practice of infectious diseases. 2010. [Google Scholar]
Article Metrics
- Visibility 8 Views
- Downloads 3 Views
- DOI 10.18231/pjms.v.15.i.1.88-92
-
CrossMark

- Citation
- Received Date February 28, 2024
- Accepted Date April 08, 2024
- Publication Date March 12, 2025