Panacea Journal of Medical Sciences
Panacea Journal of Medical Sciences (PJMS) open access, peer-reviewed triannually journal publishing since 2011 and is published under auspices of the “NKP Salve Institute of Medical Sciences and Research Centre”. With the aim of faster and better dissemination of knowledge, we will be publishing the article ‘Ahead of Print’ immediately on acceptance. In addition, the journal would allow free access (Open Access) to its contents, which is likely to attract more readers and citations to articles published in PJMS.Manuscripts must be prepared in accordance with “Uniform requiremen...

Fracture shaft femur in children –Role of titanium elastic nails in surgical management
Abstract
Background: Femoral fractures are common among children and adolescents. Its management has several methods which have improved with time recently. Most of these fractures are effectively managed conservatively with hip spica in very young children and only unstable and displaced fractures need surgical intervention. Children and adolescents in the age group of 4-19 years are treated with various methods of treatment. We have studied the short term results of femur fracture in children and adolescents prospectively which were managed by using Titanium Elastic Nailing System.
Materials and Methods: This is a short term prospective study conducted in our department of Orthopaedics, of our hospital. Forty patients aged 4-19 years, with fracture of the shaft of femur were managed by closed reduction and internal fixation with flexible titanium elastic nailing system. All the patients were followed up clinically as well as radiologically, at two weeks interval for 8 weeks, then every 4 weeks till radiological evidence of bony union.
Results: The outcome evaluation was using Flynn’s criteria of scoring system. The results were excellent in thirty seven patients (92.5%), satisfactory in three patients (7.5%) and poor in none of the case.
Conclusion: The treatment of femur fracture by using Titanium Elastic Nailing System has got distinct advantages over other methods of treatment in the age group of 4-19 years. Few of the advantages being rapid union and mobility, less operative time and less hospital stay.
Introduction
In children, up to 2% of all fractures are found to be of femoral shaft. Literature suggests it to be more common in the male gender. [1]
Its management is usually related to the age of the patient and is also influenced by other factors like the type of the fracture, whether open or closed, displaced or undisplaced, associated other fractures. In children there is often formation of good callus and they have good potential for remodeling of bone, hence most of these fractures are managed by spica cast immobilization with excellent results in young children. [2], [3] The various methods of surgical intervention include femoral shaft plating, interlocking intramedullary nail and external fixator mainly in case of open fractures. [4]
The different intervention techniques have associated inherent complications like epiphysiodesis, AVN of the femoral head etc. For the management of these fractures in children and adolescents in the age group 4-19 years, there are a vast variety of techniques with no consensus among the treating orthopaedic surgeons about the best way of management. [5] Titanium elastic nailing system (TENS) is a simple surgical procedure which gives excellent results in femoral shaft fractures. [6]
Materials and Methods
All the forty patients in the age group of 4 to 19 years who sustained and were admitted with radiological evidence of fracture of the femoral shaft were included in our research. Open fractures only of type I and II were included whereas those with more severe type III open, comminuted fractures and those where surgical procedure was contraindicated were excluded. Routine preoperative blood and radiological investigations were undertaken after recording a thorough history into the mechanism of injury.
Pre anesthetic evaluation was done and patients were prepared for surgery. Flexible titanium elastic nails of all sizes were kept ready per operatively depending upon the size of the medullary canal of the femur. All the surgical procedures were done with the patient under general anesthesia and patient lying supine over the fracture table. Parts were prepared from groin up to the mid calf region. Intravenous antibiotics were given and the entry point assessed on the c-arm. Incisions were marked vertically on medial and lateral aspect on the distal femur such that the physis is well protected from any surgical injury. Entry point is made at the same level well above the physis on either side and medullary canal is opened using an awl or a small drill bit. Minimum of two nails were inserted from distal to proximal direction. The size of the nails was selected depending upon the size of the medullary canal at its narrowest part. It is made sure that at least 4/5th of the diameter of the medullary canal is filled with the flexible elastic nails. Flynn et al’s criteria for calculating the size of the nail (Nail diameter = Width of the medullary canal at the level of isthmus on Antero posterior and Lateral view x 0.4mm). The nails were advanced proximally to well within one cm of proximal femoral physis taking care not to breach the physis. Once the position of both elastic nails is confirmed using an image intensifier, the nails are bent and cut leaving around one to two cm outside the bone so that after union of the fracture, their removal is unhindered.
The surgical procedure on an average lasted for about forty five to sixty minutes. All the patients were started on physiotherapy with knee range of motion and quadriceps exercises. Post-operative radiological evaluation was done and patients were advised to follow up after fifteen days and discharged on oral antibiotics.
All the patients were evaluated clinically for stiffness of the knee joint and radiologically at the fracture site for position of fragments, callus formation and signs of union. Weight bearing was allowed once there was radiological evidence of good callus and fracture union. The evaluation of results in each case was done using Flynn et al. criteria for evaluation. [7] ([Table 1]) All the patients were followed up for an average of twenty months. Most of the implants were removed between six to twelve months.
|
Result |
Excellent |
Satisfactory |
Poor |
|
Limb length inequality |
< 1.0 cm |
< 2.0 cm |
> 2.0 cm |
|
Malalignment |
5 degrees |
10 degrees |
>10 degrees |
|
Pain |
None |
None |
Present |
|
Complication |
None |
Minor and resolved |
Major and lasting |
Results
This is a prospective study of forty patients of femur shaft fracture who were treated with closed reduction and intramedullary nailing using titanium elastic nails of varied diameter. A minimum of two nails were inserted in each case. Age distribution among four to nineteen years age is as shown in the [Table 2], wherein it is evident that the fracture is more common in age group of nine to twelve (18/40) (45.0%) years, followed by 13-19 year age (12/40, 30.0%). The youngest child was four years old and eldest one was nineteen years old. The mean age of the study population was 10.2 years. Sex distribution as shown in [Table 3] demonstrates a male preponderance (24/40, 60.0%).
|
Age group in years |
No. of patients |
Percentage (%) |
|
04-08 |
10 |
25.0 |
|
09-12 |
18 |
45.0 |
|
13-19 |
12 |
30.0 |
|
Total |
40 |
100.0 |
|
Sex |
No. of patients |
Percentage (%) |
|
Male |
24 |
60.0 |
|
Female |
16 |
40.0 |
|
Total |
40 |
100.0 |
The most common mechanism of injury was a road traffic accident (24/40, 60.0%), followed by fall during play (10/40, 25.0%) as seen in [Table 4]. The right femur fracture was noted in 55% (22/40) of cases, [Table 5].
|
Nature of injury |
No. of patients |
Percentage (%) |
|
Road traffic accident |
24 |
60.0 |
|
Fall while play |
10 |
25.0 |
|
Fall from a height |
06 |
15.0 |
|
Total |
40 |
100.0 |
|
Side |
No. of patients |
Percentage (%) |
|
Right |
22 |
55.0 |
|
Left |
18 |
45.0 |
|
Total |
40 |
100.0 |
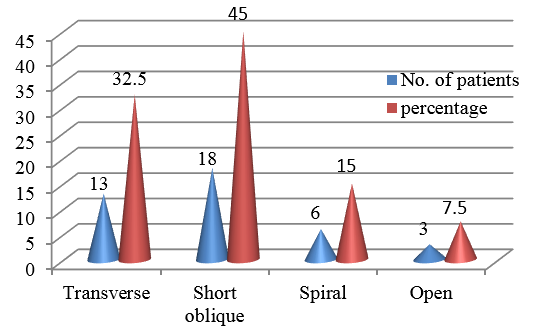
The most common pattern of injury as shown in [Figure 1], is a short oblique fracture (18/40, 45.0%) followed by a transverse fracture (13/40, 32.5%). Spiral fractures were seen in six (15.0%) of cases and open fractures were seen only in three (7.5%) cases, which were type I open fractures.
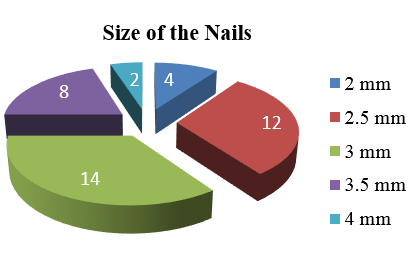
All the cases were operated within three days of injury hence we were able to achieve closed reduction. Nails of 3mm diameter were used in most of the cases (14/40, 35.0%) as is evident from [Figure 2]. The various size nails used range from two mm to four mm.
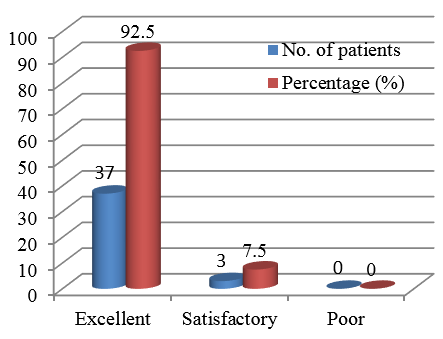
The average stay in the hospital was for seven days, and the range was three to twelve days. The mean time for radiological union was ten weeks after which weight bearing was started. The functional outcome of the study as were evaluated by Flynn’s criteria is shown in [Figure 3], which demonstrates an excellent result in 92.50% (37/40) of cases and satisfactory in 7.50% (3/40) of cases. Few of the complications seen were nail impingement in two cases which were managed by early removal of the elastic nails as soon as clinical union was ascertained. Three patients had stiffness in knee and were successfully managed by physiotherapy and range of motion exercises. No case of infection was recorded.
Discussion
The architecture of the bone in children and adolescents vary from that in the adults. There is a growing physis, thicker periosteum, small size of the bones and difference in blood supply to various bones. All these factors are to be considered while managing fractures in this particular age group.
Conservative management using plaster of paris casting can cause various complications like shortening, angulation and rotation of the fractured bones. [8] Use of interlocking intramedullary nails as in adults result in avascular necrosis of head, early fusion of trochanteric physis and increased neck shaft angle. [9]
Management using elastic intramedullary nails prevent many complications like malunion and since they are made of titanium, there is no risk of metal sensitivity reaction. [10] Various studies have demonstrated good to excellent result of union while using elastic nails. [11]
The surgical procedure is easy to perform and provides distinctive advantages in the age group of four to nineteen years than the rigid nails used in adults. There is no injury to physis hence bone growth is not hindered, load sharing implant which maintains the reduction of the fracture till formation of callus. The reduction is maintained by three-point fixation principle. There is early formation of callus and since there is no drainage of hematoma from the fracture as it is a closed reduction, there is minimal to no risk of infection of the bone. [12]
Various literature also suggest a number of advantages of using titanium elastic nails for the management of femur shaft in the age group of four to nineteen years. [13] The mean time of radiological union in our study was ten weeks and is comparable to the study by Bagul Rahul R et al. [14] and it is 8.2 weeks in the study carried out by Vishal Kumar Mishra et al. [15] The range of motion at hip and knee following this procedure were studied by Kanthimathi et al. [16] and demonstrated full range in their study group of twenty five patients. Similar study by Flynn J Metal [17] resulted in knee stiffness in two patients which were successfully managed by manipulation of the joint under anesthesia.
The clinical and functional result of our study is comparable to those demonstrated by Mohit Khanna et al. [18] and Avinash Pulate et al. [19] Study conducted by Saurabh Gupta et al. [20] had mild complications in twenty five percent of their study group. Divesh Jalan et al. [21] in their study recorded six cases of irritation of the elastic nail entry point.
Flynn et al. [22] conducted similar study on a large group of about two hundred and thirty four fractures and recorded only minor angulation deformity. Our study has no case of either shortening or angulation deformity. Singh et al. [23] in his study recorded few cases of angulation deformity in both coronal and sagittal plane.
Conclusion
Management of femur shaft fractures using intramedullary flexible titanium elastic nails in children and adolescents of age group four and nineteen has many advantages when compared to other methods and is the best method to achieve excellent clinical and functional results.
Source of funding
None.
Conflict of Interest
None.
References
- Loder R, O'Donnell P, Feinberg J. Epidemiology and mechanisms of femur fractures in children. J Pediatr Orthop. 2006;26(5):561-6. [Google Scholar]
- Irani R, Nicholson J, Chung S. Long-term results in the treatment of femoral-shaft fractures in young children by immediate spica immobilisation. J Bone Joint Surg Am. 1976;58(7):945-51. [Google Scholar]
- Henderson O, Morrissy R, Gerdes M, Mccarthy R. Early casting of femoral shaft fractures in children. J Pediatr Orthop. 1984;4(1):16-21. [Google Scholar]
- Skak S, Overgaard S, Nielsen J, Andersen A, Nielsen S. Internal fixation of femoral shaft fractures in children and adolescents: a ten- to twenty-one-year follow-up of 52 fractures. J Pediatr Orthop B. 1996;5(3):195-9. [Google Scholar]
- Clinkscales C, Peterson H. Isolated closed diaphyseal fractures of the femur in children: comparison of effectiveness and cost of several treatment methods. Orthopedics. 1997;20(12):1131-6. [Google Scholar]
- Hedin H. Surgical treatment of femoral fractures in children. Comparison between external fixation and elastic intramedullary nails: a review. Acta Orthop Scand. 2004;75(3):231-40. [Google Scholar]
- Flynn J, Hresko T, Reynolds R, Blasier R, Davidson R, Kasser J. Titanium elastic nails for pediatric femur fractures: a multicenter study of early results with analysis of complications. J Pediatr Orthop. 2001;21(1):4-8. [Google Scholar]
- Martinez A, Carroll N, Sarwark J, Dias, L, Kelikian A, Jr GS. Femoral shaft fractures in children treated with early spica cast. J Pediatr Orthop. 1991;11(6):712-6. [Google Scholar]
- Beaty J, Austin S, Warner W, Canale S, Nichols L. Interlocking intramedullary nailing of femoral shaft fractures in adolescence: preliminary results and complications. J Pediatr Orthop. 1994;14(2):178-83. [Google Scholar]
- Ligier J, Metaizeau J, Prevot J, Lascombes P. Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br. 1988;70(1):74-7. [Google Scholar]
- Kanthimathi B, Kaliya-Perumal A. Flexible Intramedullary Nailing for Paediatric Shaft of Femur Fractures – Does the Number of Nails Alter the Outcome?. Malaysian Orthop J. 2011;5(2):28-33. [Google Scholar]
- Gwyn D, Olney B, Dart B, Czuwala P. Rotational control of various pediatric femur fractures stabilized with titanium elastic intramedullary nails. J PediatrOrthop. 2004;24(2):172-7. [Google Scholar]
- Flynn J, Skaggs D, Sponseller P, Ganley T, Kay R, Leitch K. The Operative Management of Pediatric Fractures of the Lower Extremity. J Bone Joint Surg Am. 2002;84(12):2288-300. [Google Scholar]
- Rahul B, SB, Pramod P, DS, Vivek P, Swaroop S. Surgical management of fracture shaft femur in children and adolescents with titanium elastic nailing system. Int J Orthop Sci. 2017;3(4):330-5. [Google Scholar]
- Mishra V, Kumar A, Kumar G, Sarang S. Functional Outcome Of Fracture Shaft Of Femur In Pediatric Age Group Treated With Titanium Elastic Nailing System. Int J Med Biomed Stud (IJMBS). 2020;4(1):175-9. [Google Scholar]
- Kanthimathi B, Kumar K. Flexible Intramedullary Nailing for Paediatric Shaft of Femur Fractures-Does the Number of Nails Alter the Outcome. Malaysian Orthop J. 2011;5(2):28-33. [Google Scholar]
- Flynn J, Skaggs D, Flynn J, DS, PW. Femoral shaft fractures. Rockwood & Wilkins’ Fractures in Children. 2014. [Google Scholar]
- Khanna M, Wadhwani J, Batra A, SY, Iman S, Vashishth S. Tens For The Surgical Management Of Femoral Shaft Fractures In 6-14 Years Age Group Children. Pediatr Traumatol Orthop Reconstr Surg. 2017;5(2):13-21. [Google Scholar]
- Pulate A, Jadhav A, Shah B. Study of the Outcome of Titanium Elastic Nail System in Diaphyseal Femoral Fractures in Children . J Maharashtra Orthop Assoc. 2012;7(3):6-8. [Google Scholar]
- Gupta S, Hegde J. Prospective Study of Management of Diaphyseal Fractures of Femur in Paediatric Age Group by Titanium Elastic Nailing System. J Med Thesis. 2024;2(1):19-23. [Google Scholar]
- Jalan D, Chandra R, Sharma V. Results of titanium elastic nailing in paediatric femoral diaphyseal fractures----report of 30 cases. Chin J Traumatol. 2013;16(2):77-83. [Google Scholar]
- Flynn J, Luedtke L, Theodore J, Dawson J, Davidson R, Dormans J. Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am. 2004;86(4):770-7. [Google Scholar]
- Singh J, Virk J, Kalia A, Mittal N. Flexible intramedullary nails: the panacea for paediatric femoral shaft fractures. Int J Res Orthop. 2017;3(3):411-6. [Google Scholar]
Article Metrics
- Visibility 7 Views
- Downloads 2 Views
- DOI 10.18231/pjms.v.15.i.1.158-162
-
CrossMark

- Citation
- Received Date September 01, 2024
- Accepted Date November 09, 2024
- Publication Date March 12, 2025